A Word Problem
Jan 25, 2024
I have a word problem. The words are Disorder, Deficit, Disability, and Disease. They all start with the letter D but that’s just a coincidence.
Let me take a step back. I’m a neurodivergent person. I’m dad to a neurodivergent kid, husband to a neurodivergent spouse, brother to a neurodivergent sibling, child of neurodivergent parents, and teacher of some wonderful neurodivergent kids.
So what does this word ‘neurodivergent’ mean? Neurodiversity is a concept first articulated by Australian sociologist Judy Singer in 1997[1]. It’s the idea that, just as a variety of organisms fill the ecological niches in a given biome, many different types of human brains, optimized for different ways of thinking, co-exist in any group of people of sufficient size. Despite this diversity, most brains tend to fall within an arbitrary set of boundaries considered ‘typical’, and thus ‘neurotypical’. The brains that fall outside of those boundaries? Neurodivergent.
Psychology, in its neverending zeal to label and organize (cf. The DSM-5), has lots of terms to describe various presentations of neurodivergence: Autism Spectrum Disorder, Attention Deficit Hyperactivity Disorder, Tourette Syndrome, Obsessive Compulsive Disorder, Dyslexia, Dyspraxia, Intellectually Gifted, Bipolar Disorder, Anxiety Disorder.
I sense a pattern (something neurodivergent brains are often particularly good at). A lot of those D words appear in this list. Why does it matter? Because the words we use to describe ourselves and others affect how we think and feel about ourselves and others.
I recently read the brilliant novel Cassandra in Reverse by Holly Smale. This quote stopped me in my tracks:
“Other people’s words about me became how I saw me too.”[2]
That’s something I’ve experienced in my life. I bet a lot of other neurodivergent people (and people belonging to marginalized groups in general) have experienced that too.
So, why do we call Autism a disorder? Why do we say people with ADHD have an attention deficit (when they clearly have an overabundance of attention for the things they care about)? Why do we diagnose dyslexia without also diagnosing hyper-creativity when studies have found that dyslexic people are likely to have above average creative and artistic abilities?[3]
Homosexuality was labeled a disorder in the DSM until 1974. It was only with the publication of the DSM-5 in 2014 that diagnostic categories applicable to people based on their sexual orientation were finally removed. If you look at the world through a biased lens, arbitrarily holding up yourself as the norm, assuming anyone who looks, acts, or thinks differently from you is wrong, you will find disorder and deficit everywhere.
As a parent, a teacher, and a coordinator of an affinity group for neurodivergent students, I’ve talked to a lot of kids who have had the natural, amazing way their brains work labeled a ‘disorder’ or a ‘deficit’, in the same way that homosexual and trans kids used to have their natural, normal sexuality and gender identities labeled as disorders. That language hurts. That language can destroy self-esteem. That language may be partially responsible for the tragically high rate of suicide among neurodivergent kids.
I’m not saying that these brain differences are not often disabling. They definitely can be, especially when neurodivergent people are placed in situations where neurotypical behavior and abilities are expected and no accommodations are provided: an ADHD child in a typical classroom, an autistic person in an unstructured social setting, a dyslexic person with a dense text to read, a dyspraxic student in a standard PE class.
The D words are not the only issues with the DSM diagnoses though. There’s another big problem: Aside from the harm they can cause, they are just not very useful to the person receiving the diagnosis. Telling me my child has ASD or ADHD, handing me a dry, multi-page explanation full of specialized vocabulary along with (if I’m lucky) a referral for OT or (if I’m unlucky) ABA assessment, and sending me on my way is only helpful in the narrowest of possible interpretations of ‘helpfulness’. As a parent, this has happened to me twice and I have met many other parents who have shared the same experience.
Not to go too deep, but the DSM seems to me to be a classic example of what Audre Lorde called the master’s tools. If, as neurodivergent people, we consent to go on existing within the limiting paradigm of the DSM, we will never have the capacity to bring about genuine change. In Lorde’s words: “Only the most narrow parameters of change are possible and allowable” when we accept the limitations of the master’s tools. To make real change, we have to step out of that paradigm and learn to see our difference as strength. [4]
As I often tell my students, though, we shouldn’t criticize if we aren’t ready to offer an alternative. So, here is my modest proposal for a system that would work better. This is similar, in a way, to the RDoC project which exists as a kind of antidote to the DSM5 but it's much simpler, aimed specifically at neurodivergence, and also rejects the very idea of diagnosis.
Imagine a child is struggling in school. They are referred for neuropsychological testing. But, instead of their parents walking out with a piece of paper listing their child’s deficits and disorders, they walk out with a paper listing their child’s individual traits and an indication of where they fall on a continuum of other people. Some of those traits might be disabling in some situations. Some of them might be enabling. For example (assuming M is the median or ‘neurotypical’ range):
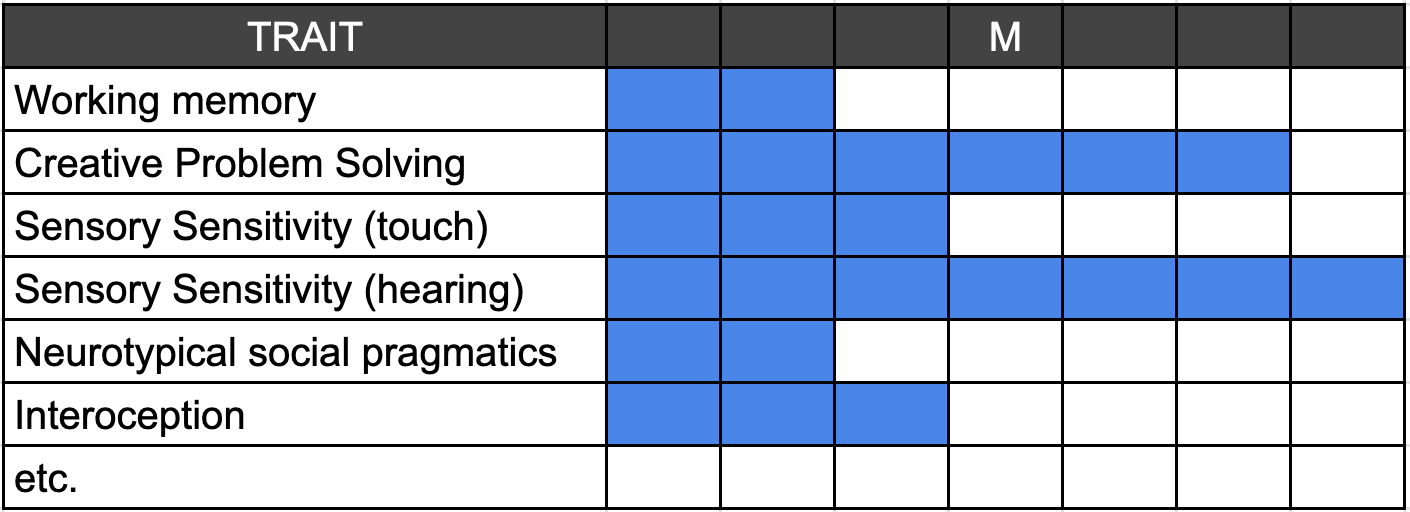
Why would this be better? Because it’s (1) actionable and (2) less stigmatizing. Rather than bewildered parents, teachers, and school administrators facing a confusing landscape of IEPs, decisions about adopting various therapies (that often have no objectively verifiable efficacy), battles for accommodation, and poorly understood challenges, we could have a clear roadmap for how to support a child.
Did the testing show that a child has a high sensitivity to sound? Try getting them some noise canceling headphones. Selective mutism? Understand that they can’t speak sometimes and develop other ways to communicate when that occurs. High spacial reasoning ability? Help steer them toward activities where this ability is recognized and nurtured.
Would this mean doing away with official diagnoses? No. Official diagnoses are unfortunately still necessary to qualify for services within the health insurance and public school systems. It could be a very useful addendum though–one that recognized the complex reality of neurodivergence. Most neurodivergent people’s traits do not fit neatly in the ASD box or the ADHD box or the OCD box. Given that so many people who meet the criteria for one diagnosis also meet the criteria for others[5] [6], it might be time for the psychological community to start thinking of neurodivergence not as a list of DSM diagnoses full of D words, but as individual traits all existing on their own separate continua.
For example: Two of my family members can’t distinguish faces. This is called prosopagnosia in the DSM. It’s far more common in neurodivergent people than in the general population[7] but it was not identified in any of their neuropsychological testing. Why? The people administering the testing didn't bother looking. It’s actually a much more disabling trait than most of the others we could add to our list of neurodivergent traits but the psychologists were focused on the narrow list of diagnostic criteria contained in the DSM-5 rather than looking at the whole picture.
Things like this wouldn’t be missed if we focused on a broad range of traits rather than a narrow band of ‘symptoms.’ Which traits do you have? Put them together and that’s your own brand of neurodivergence. Investigate them all and figure out how to accommodate, benefit from, nurture, or work around them. Give people an individualized operating manual for their mind, not an acronym fulls of Ds.
I have approached this essay from the perspective of a parent and teacher but everything I have written should be equally applicable to an adult who has received a diagnosis or self-diagnosed (equally valid). The psychologists and psychiatrists can keep their diagnoses if they must but let’s please find new words to replace all the Ds. Additionally, let’s find a way to add actionable, holistic data. Instead of stop signs and dead ends, Let’s provide detailed maps of the terrain ahead to help people navigate their neurodivergent journeys.
[1] Harris, J. (2023, July 5). The Guardian. https://www.theguardian.com/world/2023/jul/05/the-mother-of-neurodiversity-how-judy-singer-changed-the-world
[2] Smale, H. (2023). Cassandra in Reverse (1st ed., p. 347). Harper Collins.
[3] Taylor, H., & Vestergaard, M. (2022). Developmental Dyslexia: Disorder or Specialization in Exploration? Frontiers in Psychology, 13(2022). https://doi.org/10.3389/fpsyg.2022.889245
[4] Lorde, Audre. “The Master’s Tools Will Never Dismantle the Master’s House.” 1984. Sister Outsider: Essays and Speeches. Ed. Berkeley, CA: Crossing Press. 110-114. 2007. Print.
[5] Brimo, K. (2021). The co-occurrence of neurodevelopmental problems in dyslexia. Dyslexia, An International Journal of Research and Practice, 27(3). https://doi.org/10.1002/dys.1681
[6] ASD and ADHD Comorbidity: What Are We Talking About? Front Psychiatry. 2022; 13: 837424. Published online 2022 Feb 28. doi: 10.3389/fpsyt.2022.837424
[7] Minio-Paluello, I., Porciello, G., Pascual-Leone, A. et al. Face individual identity recognition: a potential endophenotype in autism. Molecular Autism 11, 81 (2020). https://doi.org/10.1186/s13229-020-00371-0